

TMJ Joint Pain
TMJ pain can be broken down into 2 separate causes:
-
Internal Joint Problems
-
Non-Joint problems affecting the joint
There are 5 main parts of the TMJ: Bones, Disk, Capsule, Nerves/Blood Vessels and Muscle
TMJ pain is extremely complex. Contrary to what many people believe TMJ joint is usually not the cause of the pain. 80 to 90% of people with TMJ pain have a muscle problem, not a joint problem. This is a good thing because it means invasive procedures will not be necessary. Muscle problems are solved by relaxing the muscles (see muscle pain for more).
Intrinsic TMJ joint problems stem from the very complex nature of the TMJ. In order to understand TMJ pain, you should first understand the anatomy of the TMJ. The TMJ has 5 main parts: The bony joint, the disk, the soft tissue capsule the nerves/blood vessels and muscles.
The Bones of the TMJ
Bone Motion:
The TMJ is very unique. It is the only joint in the body that consists of a rotation motion as well as a sliding motion. The first 15mm (about 1 finger breadth) of opening are a rotation movement within the mandibular fossa. All remaining opening is done by a sliding motion up a ramp called the TMJ eminence.
The Mandibular Condyle:
The mandible is the lower jaw bone. The Jaw bone is shaped like a "U" with each side ending in what is known as the condyle. The condyle is made of dense bone called cortical bone on the outside and soft bone called cancellous bone on the inside. This is the "ball" in the "ball and socket" joint analogy.
The TMJ Fossae:
The fossa is the socket of the joint. It is also made of dense cortical bone on the outside to resist wear and act as a hard "stop" for the jaw to rest on. The fossae is naturally smooth and rounded leading up to a slope called the "eminence" (which means bump).
The TMJ Eminence:
The TMJ eminence is the most forward (anterior) part of the joint. It consists of a sloping ramp of bone that the condyle slides up when you open large (anything past about one finger breadth of opening).

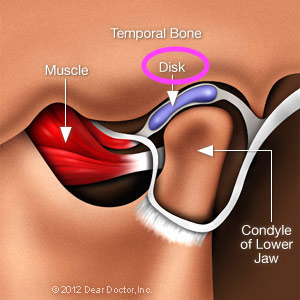
The Disk of the TMJ
The Disk of the TMJ is a small disk of cartilage that rests between the condyle and the TMJ fossa in a resting position (it separates the ball from the socket). The Disk then slides forward and up the ramp of the TMJ eminence upon opening. A healthy disk is always separating the bones. A diseased disk is often slipped forward or has a hole in it. When you hear clicking or popping in your jaw, it is from the condyle of the mandible clicking on and off the disk as you open. When you have closed mouth lock or inability to open very wide it is from this bunched up disk being pushed up forward and not allowing the condyle to slide up the ramp of the eminence.
The Capsule of the TMJ
The TMJ Capsule
The capsule of the TMJ is a tough fibrous capsule that surrounds the bones, disk, nerves and vessels. Normally the capsule's job is to keep things tight and tidy. It helps to keep the disk in place and hold the fluid in place that lubricates the joint (called synovial fluid). When the disk gets too stretched from a disk that is displaced or becomes inflamed from constant tension it becomes tender. This inflammation is called capsulitis.


The Nerves and Vessels of the TMJ
The Retrodiscal tissue:
The nerves and vessels of the TMJ are mostly located in what is called the "retrodiscal tissue" (ie. the tissue behind the disk). The retrodiscal tissue is the major cause of your pain in a painful joint. This arrises when the disk slips forward. When the disk slips forward the retrodiscal tissue is the only tissue separating the bones of the joint. So the ball and socket are squeezing this rich area of blood vessels and nerves. Not only does this cause pain from compressing the nerves, but it also causes inflammation. The compression of the blood vessels causes a lack of blood supply to the joint (called hypoxia). This is similar to putting a tight rubber band around your wrist -- your hand will turn blue and hurt. The easy solution to this problem is taking off the rubber band. TMJ specialists primary aim is to stop this very process. Splints separate the teeth which pulls the bones off the nerves and vessels for temporary relief (similar to pulling the rubber band away from your wrist to allow some blood to flow). Surgeons physically move the disk back into place either through minimally invasive procedures like arthroscopy, or open joint procedures.
The Muscles of the TMJ
The TMJ Muscles
The muscles of the TMJ, like all it's other parts, are complex. These muscles are called the muscles of mastication (chewing muscles). The primary muscles attached to the TMJ are the lateral pterygoid muscles. These muscles attach to the condyle and to the disk. Their primary function is to stabilize the joint while opening and closing.
The other muscles associated with the TMJ are the temporalis, masseter, and medial pterygoid. These are powerful muscles that allow the jaw to close tightly to chew food. These muscles pack more force than any other in the body. That's good news for eating a steak but very bad news for a small disk that separates the bones of the TMJ. When these muscles are overused they get sore (like a weightlifter's muscles). Unlike a weightlifter who can rest, it is not natural to rest your jaw muscles because they are the most utilized in the body (talking, chewing, yawning and swallowing). These muscles never get a break unless there is a conscious effort on your part. TMJ appliances (ie splints), soft diets, muscles relaxers and anti-inflammatory medications can also be used to rest these muscles.

Classifying your TMJ Disorder
There are 5 classes of TMJ internal derangement according to the "Wilkes Classification:
Wilkes Classification of TMJ
I. Painless Clicking with no restriction of motion
Associated with a disk that has slipped forward
II. Occasionally painful clicking with intermittent locking and headaches
Associated with a disk that has slipped forward
III. Frequently pain, Joint tenderness to touch, locking and headaches
Associated with a disk that has slipped forward but doesn't ever slide back
IV. Chronic pain, headaches and crackling sound (crepitus)
Associated with disk deformity and bone changes
V. Sometimes painful, sometimes not with joint crackling (crepitus)
Severe disk deformity and bone changes
Minimally invasive treatment options (arthroscopy) have been shown to be effective in Class I, II, and III with an 80% success rate.
If you have clicking, popping, locking or frequent pain in your joint(s), you should see a TMJ specialist.
